TL;DRTemperament dwarfs everything — but religion and class fail differently.
You asked: religion vs class vs neuroticism — what actually moves PMS? The ordering is unambiguous: temperament first by a mile (neuroticism, then diagnosed mental health), religious upbringing a distant but robust third, and childhood class essentially nowhere once you account for the company it keeps. More interestingly for causality: the religion and class gradients fail different stress tests. Controlling for temperament barely dents the religion effect but guts the class effect — meaning "poor childhood → worse PMS" is mostly a proxy for worse adult mental health, while "religious childhood → worse PMS" is tracking something temperament doesn't explain.
01The chart you asked for, done properly
Your explorer view — PMS by childhood class, colored by religious upbringing — with CIs and the upbringing variable split three ways ("What religion did you grow up in?" → organized religion / none-casual / explicitly atheist):
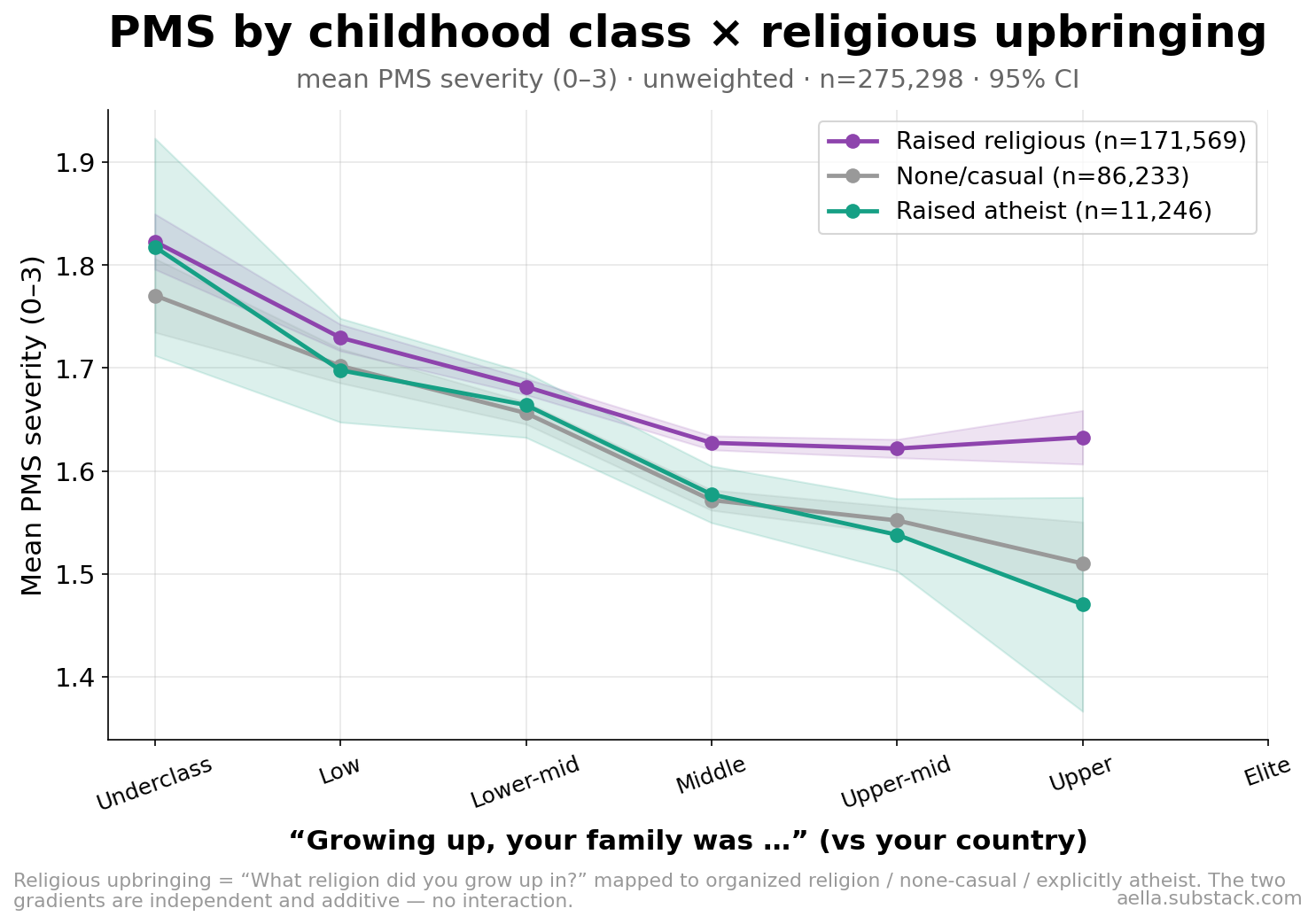
Three things to read off it: (1) the class gradient — PMS falls from underclass to upper class within every religion group; (2) the religion gap — raised-religious women sit above raised-atheists at every class level; (3) no interaction — the lines are basically parallel, so the two effects are additive: being poor doesn't make religion worse, being religious doesn't make poverty worse. They're separate (small) forces.
02What matters most: the head-to-head
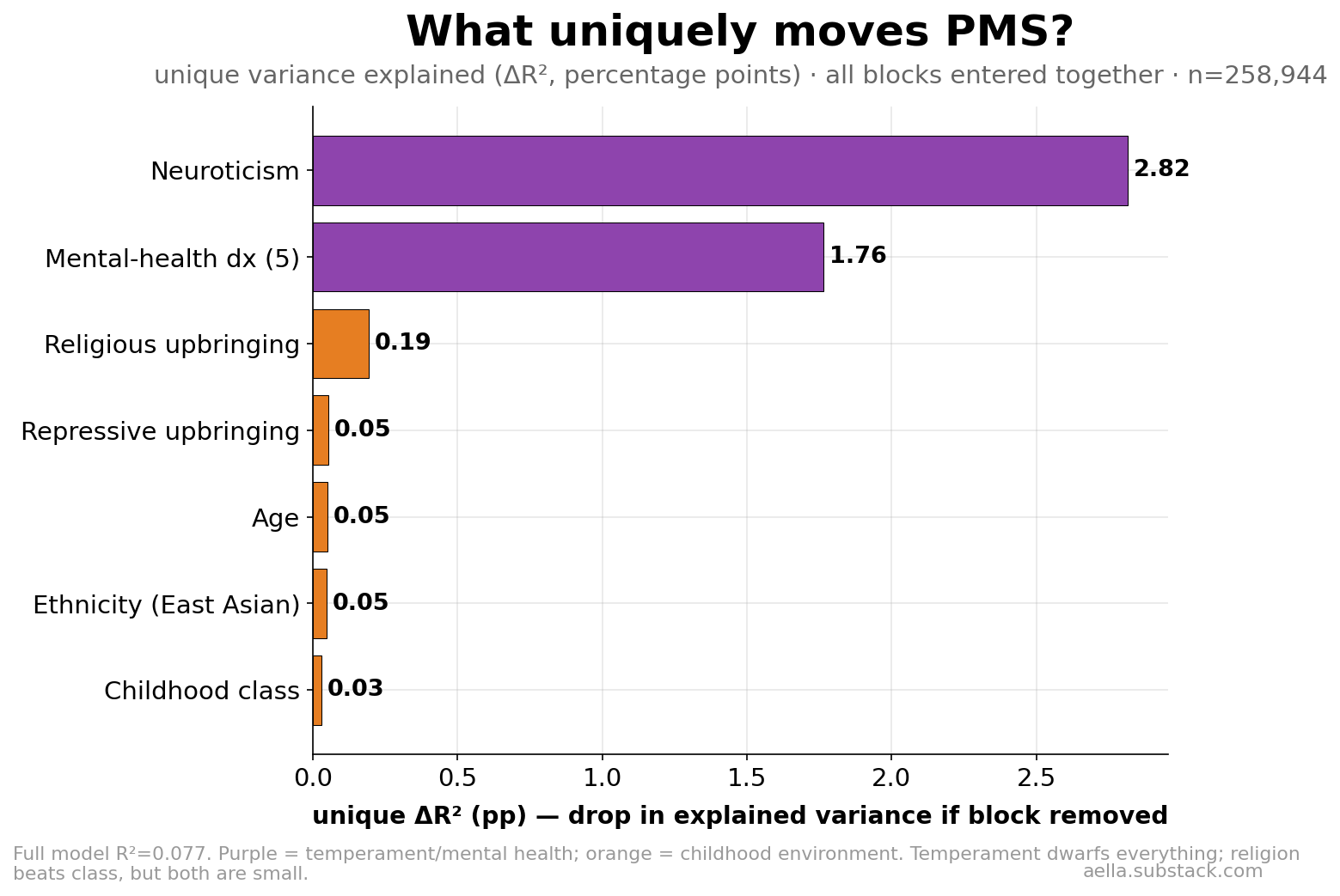
Putting every candidate in one model and asking how much explained variance each uniquely contributes (what you lose by deleting just that block):
| Block | Unique ΔR² (pp) | Read |
|---|---|---|
| Neuroticism | 2.82 | dominant |
| Mental-health diagnoses (5) | 1.76 | second, overlaps neuroticism |
| Religious upbringing (raised + intensity) | 0.19 | small but clearly nonzero |
| Repressive upbringing | 0.05 | trace |
| Age / East Asian | 0.05 each | trace |
| Childhood class | 0.03 | ~nothing unique |
So in the religion-vs-class-vs-neuroticism horse race: neuroticism ≈ 15× religion ≈ 90× class. And the whole model still explains only R²≈0.08 — most of who gets bad PMS is none of these things.
03The causal tease: watch each gradient face its controls
Cross-sectional data can't prove causation, but it can break causal stories. If "religious upbringing → PMS" were really just "religious families produce anxious women, and anxious women report PMS," then controlling anxiety/neuroticism should erase the religion coefficient. Here's each gradient as controls stack up:
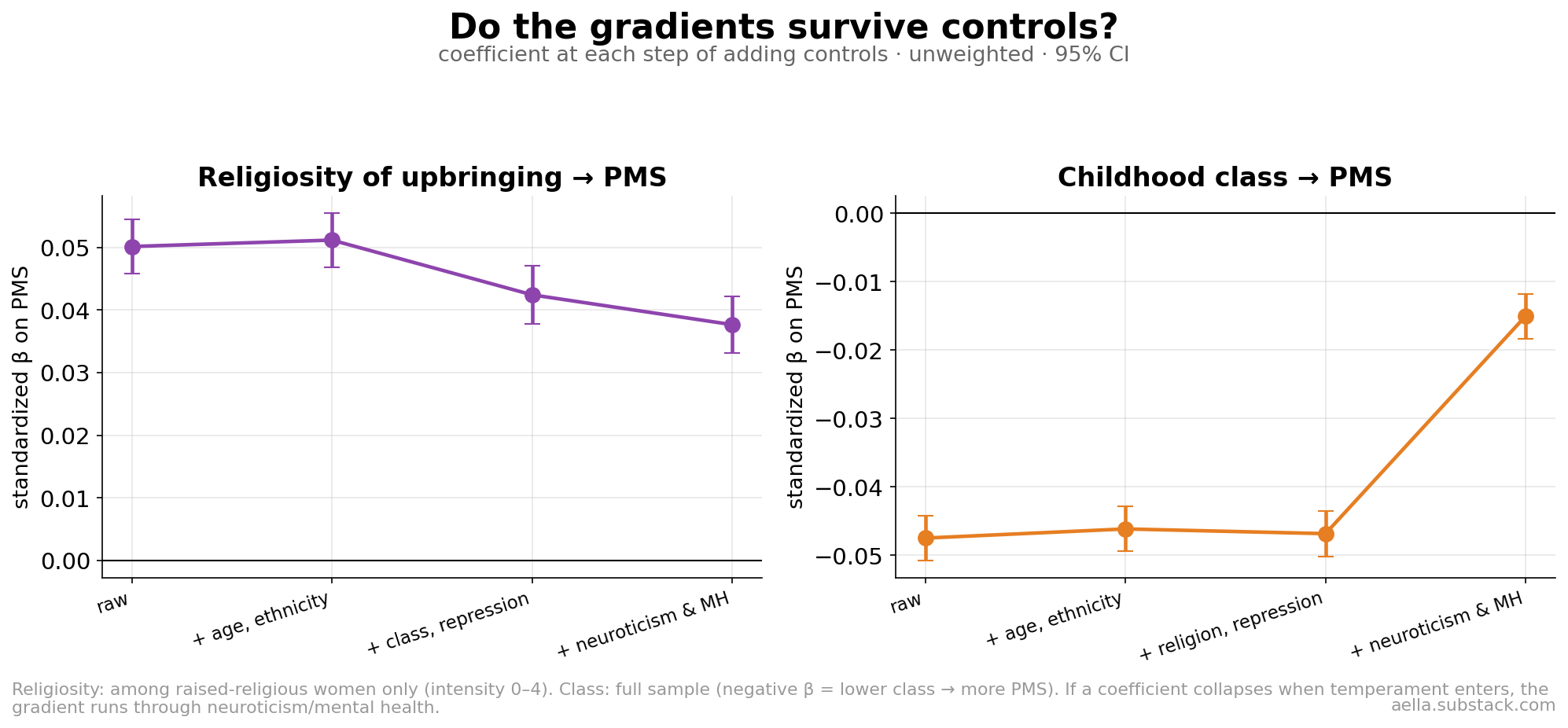
- Religiosity of upbringing (left): survives. β=0.050 raw → 0.038 with everything controlled, including neuroticism and all five diagnoses. Only ~25% of the effect runs through measurable temperament. Whatever links a heavily religious childhood to worse adult PMS, it is not mostly "religious women are more neurotic."
- Childhood class (right): collapses. β=−0.048 raw, completely indifferent to religion controls — then loses ~70% the moment neuroticism and mental health enter (→ −0.015). The class–PMS link is mostly a proxy: poorer childhoods → worse adult mental health → more reported PMS.
04Does the type of religion matter?
Mostly no. Raw differences between denominations shrink to ~nothing once you hold religiosity intensity (plus age, class, East-Asian share) constant — raised-Muslim, raised-Catholic, raised-Jewish, and raised-Protestant women all land within ±0.03 of each other. The exception is Buddhism: still −0.08 below Protestant after adjustment (partly East-Asian overlap the control may not fully absorb).
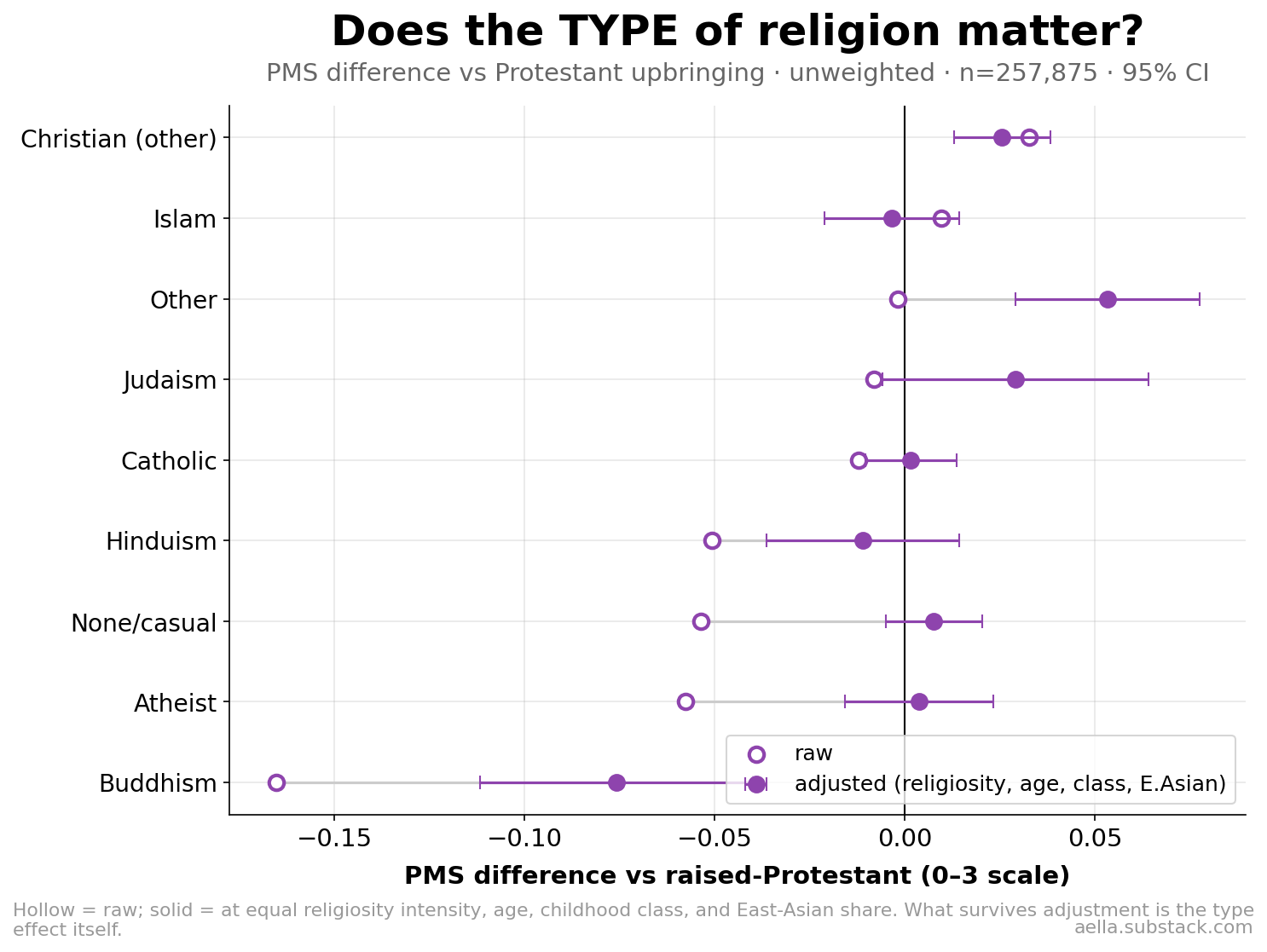
And the religiosity dose-response appears within every major denomination — more intense religious upbringing → more PMS whether the religion was Catholic, Protestant, other-Christian, Islam, or Judaism:
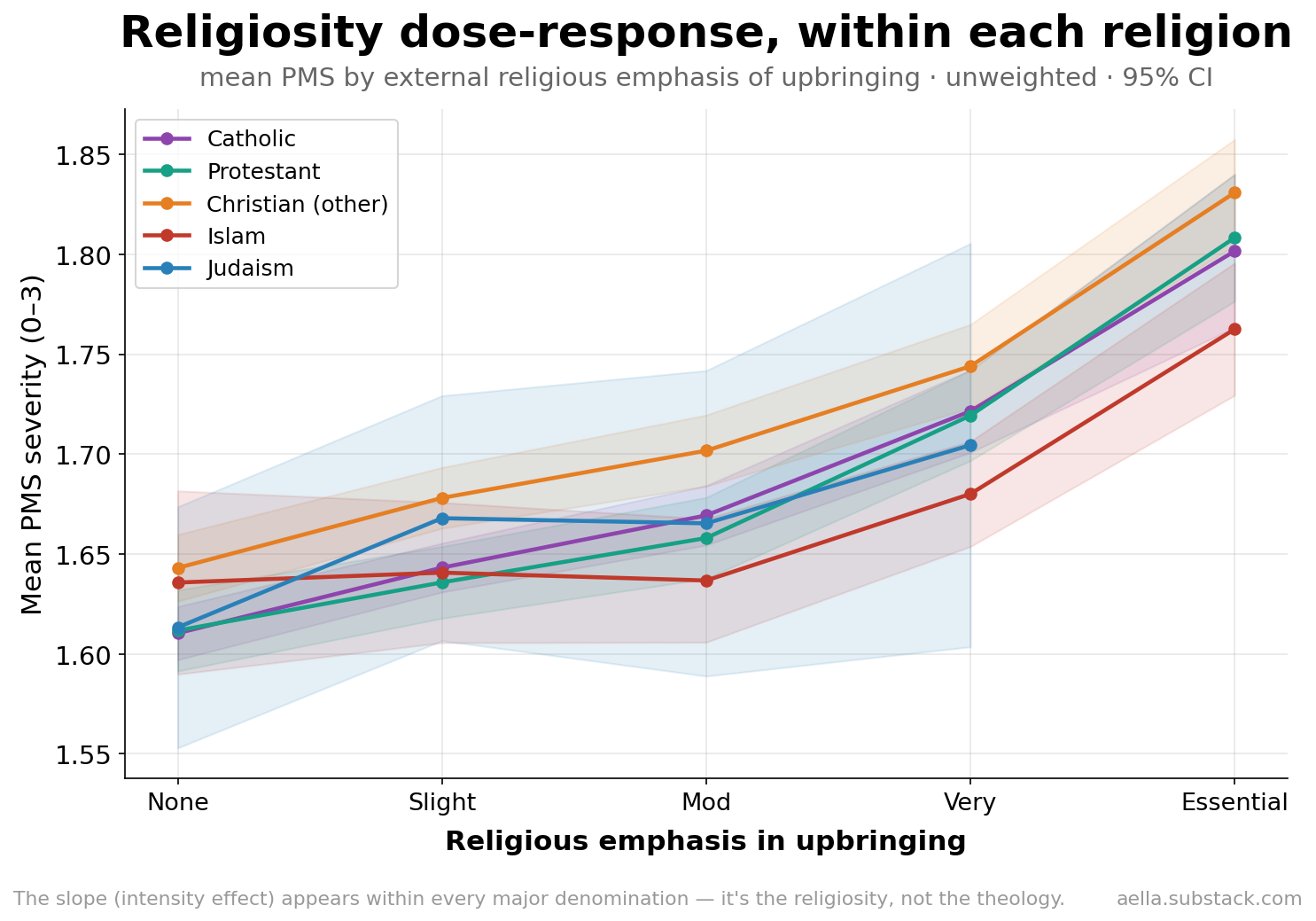
It's the religiosity, not the theology.
05Leaving the faith doesn't lower it
If current religious belief drove PMS, women who left their childhood religion should look different from those who stayed. They don't — if anything, leavers report slightly more (1.61 vs 1.57, not significant, small post-2026 subsample):
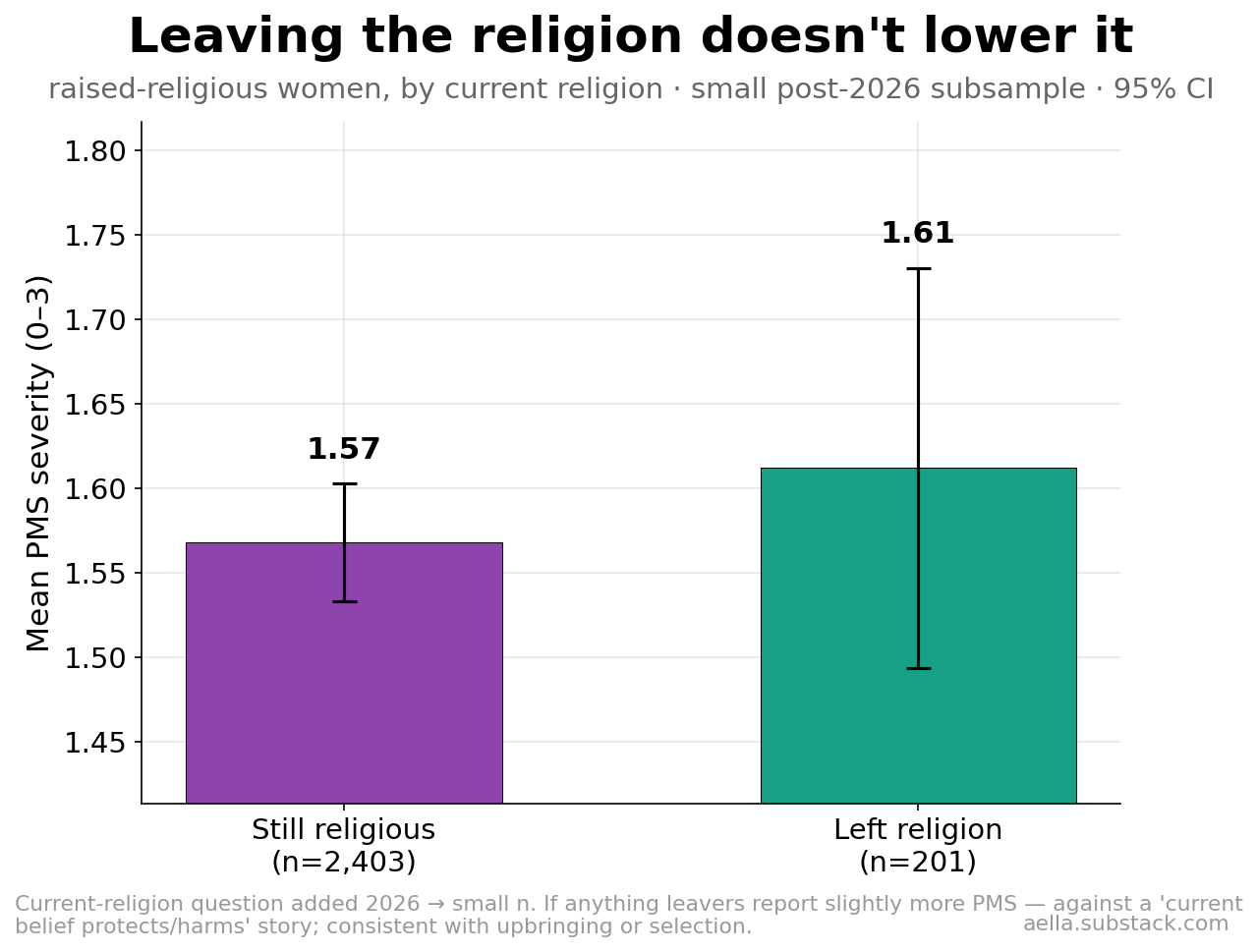
That points the arrow at the upbringing (or at whatever kind of family chooses intense religion), not at present-day belief or practice.
06So what can we actually say about causality?
Honestly, this:
- Temperament vs PMS is partly definitional — both are measured through negative mood, so neuroticism's dominance is inflated. It's still the best single predictor by far.
- Childhood class → PMS: probably not direct. It collapses under temperament controls, consistent with class affecting adult mental health, which carries the PMS report.
- Religious upbringing → PMS: a real, temperament-independent residue. It survives controls, shows dose-response, is type-invariant, and doesn't respond to leaving. Candidate explanations the data can't separate: religious upbringings teach stronger somatic/menstrual stigma (labeling); they cause lasting stress responses not captured by our MH measures; or families that choose intense religion differ in unmeasured heritable ways. What we can rule out: it's not current belief, not theology, not class, and not mostly neuroticism.
- Everything here is small. The honest headline stays R²≈0.08: PMS severity is overwhelmingly idiosyncratic — likely biological/hormonal variation this survey doesn't measure.
07Methods & limitations
Sample: BKS women (incl. NB-AFAB, excl. known-pregnant) with a PMS answer, n=275,298 unweighted (June 2026 pull, n=1,071,355 total). PMS: "Do you get mood-based PMS symptoms during your menstrual cycle?" 0–3. Religion: "What religion did you grow up in?" (+ external religious emphasis 0–4, asked of those raised in a religion). Class: "Growing up, your family was…" 0–6. Variance decomposition: OLS with all blocks, unique ΔR² = full-model R² minus R² without the block (model n=258,944). Stepped models: standardized β with cumulative control sets. Type analysis adjusts denominational means to equal religiosity/age/class/East-Asian share (reference: Protestant). Apostasy uses the current-religion item added 2026 (n=2,604 raised-religious women with both answers). All CIs 95%.
- Cross-sectional; "survives controls" constrains causal stories but cannot confirm one.
- Self-reported PMS conflates experience and labeling (the main report §4 shows labeling matters for group gaps).
- Neuroticism/MH are measured in adulthood — controlling them may over- or under-correct childhood-cause stories.
- Unweighted; self-selection into a long internet kink survey applies, especially at the religious-intensity extremes.