TL;DRNear-universal, self-reports track reality, and it's mostly idiosyncratic.
This is the long version of the PMS story. The short one: mood-based PMS is the rule, not the exception; the question genuinely measures something real (it predicts how much women's symptoms actually swing across the cycle); mental health — especially neuroticism and depression — is the strongest correlate but explains surprisingly little of the variance; and the demographic differences (ethnicity, religion, country, politics) are real but small, and partly about how readily different groups label premenstrual mood as "PMS" rather than how much they experience.
01How common is it?
Population-weighted, among women who menstruate: 8.6% report no mood PMS, 34.5% slight, 39.8% moderate, 17.1% severe. Moderate is the single most common answer; over half are at moderate-or-worse.
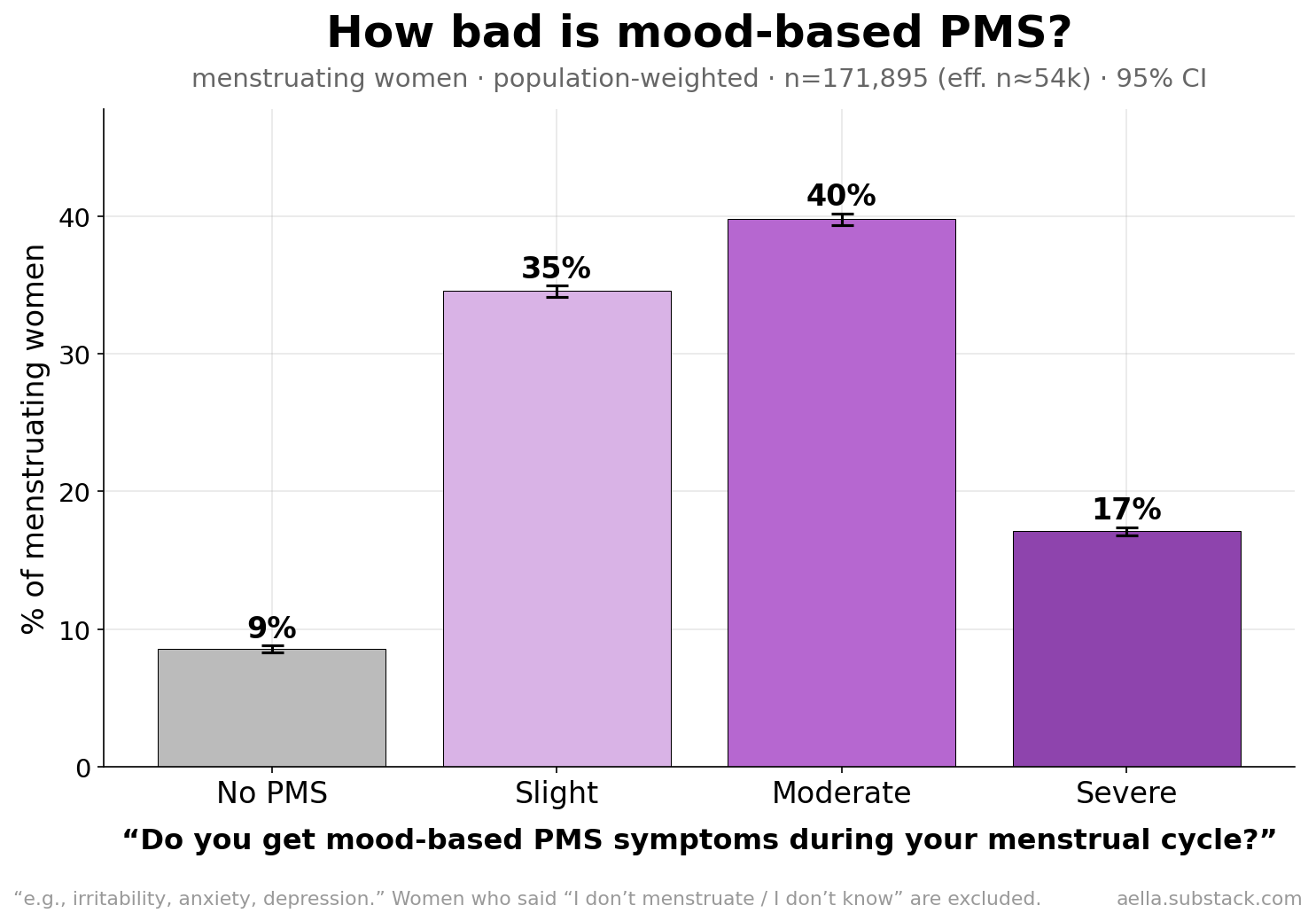
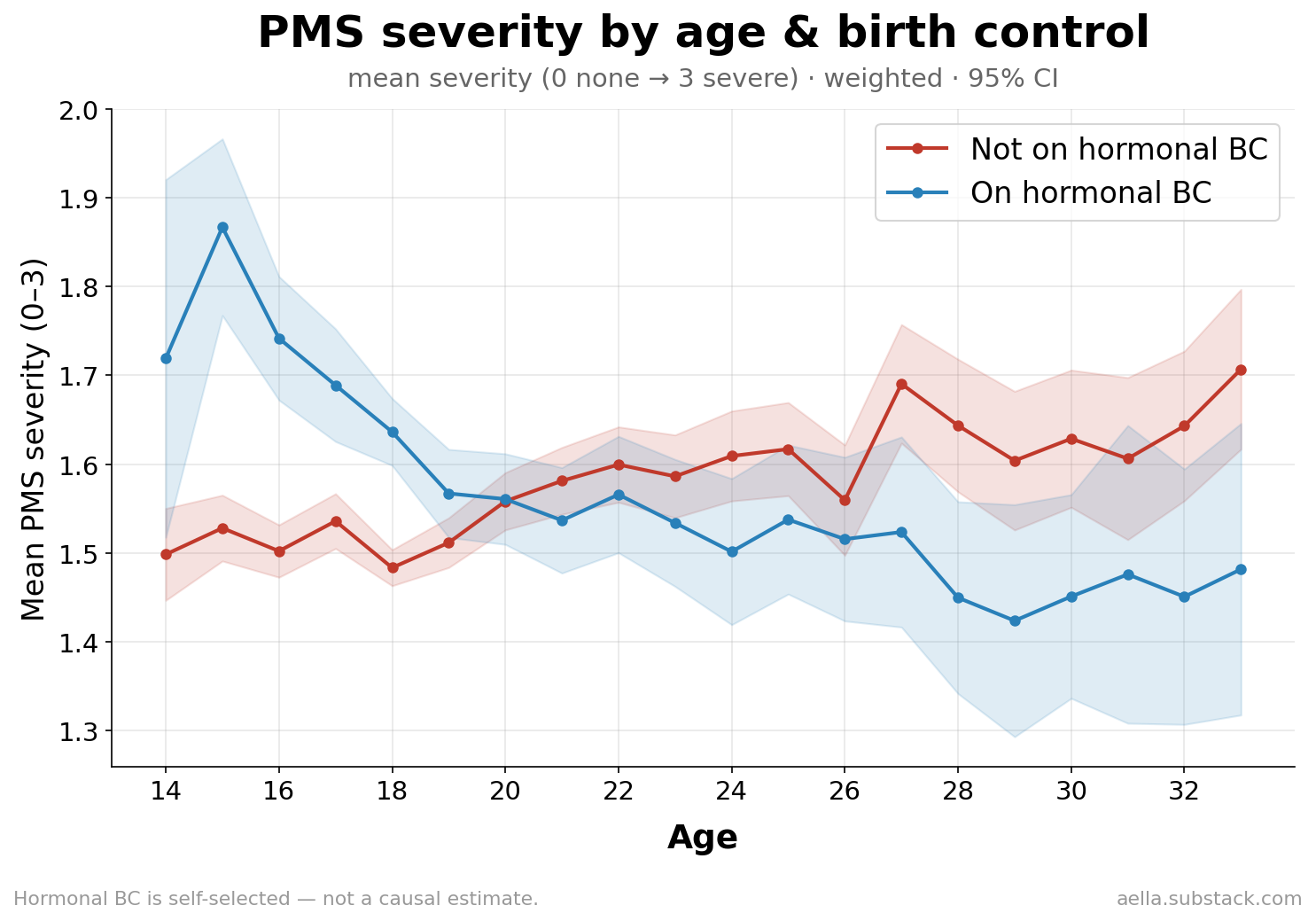
Severity drifts down slightly with age in women not on the pill; the dominant story is how stable and high it stays.
02First — does the self-report mean anything?
Before slicing it a dozen ways, it's worth asking whether "do you get mood PMS?" measures anything real or is just a personality echo. We can check, because a separate question asks women whether they're "currently experiencing PMS," and another records where they are in their cycle. If the trait question is real, women who say they get severe PMS should show a big swing in current symptoms across the cycle; women who say they get none should stay flat.
That's exactly what happens. Women reporting severe trait-PMS go from ~6% currently-symptomatic mid-cycle to ~43% pre-period — a 37-point swing. Women reporting no PMS barely move (a 4-point swing).
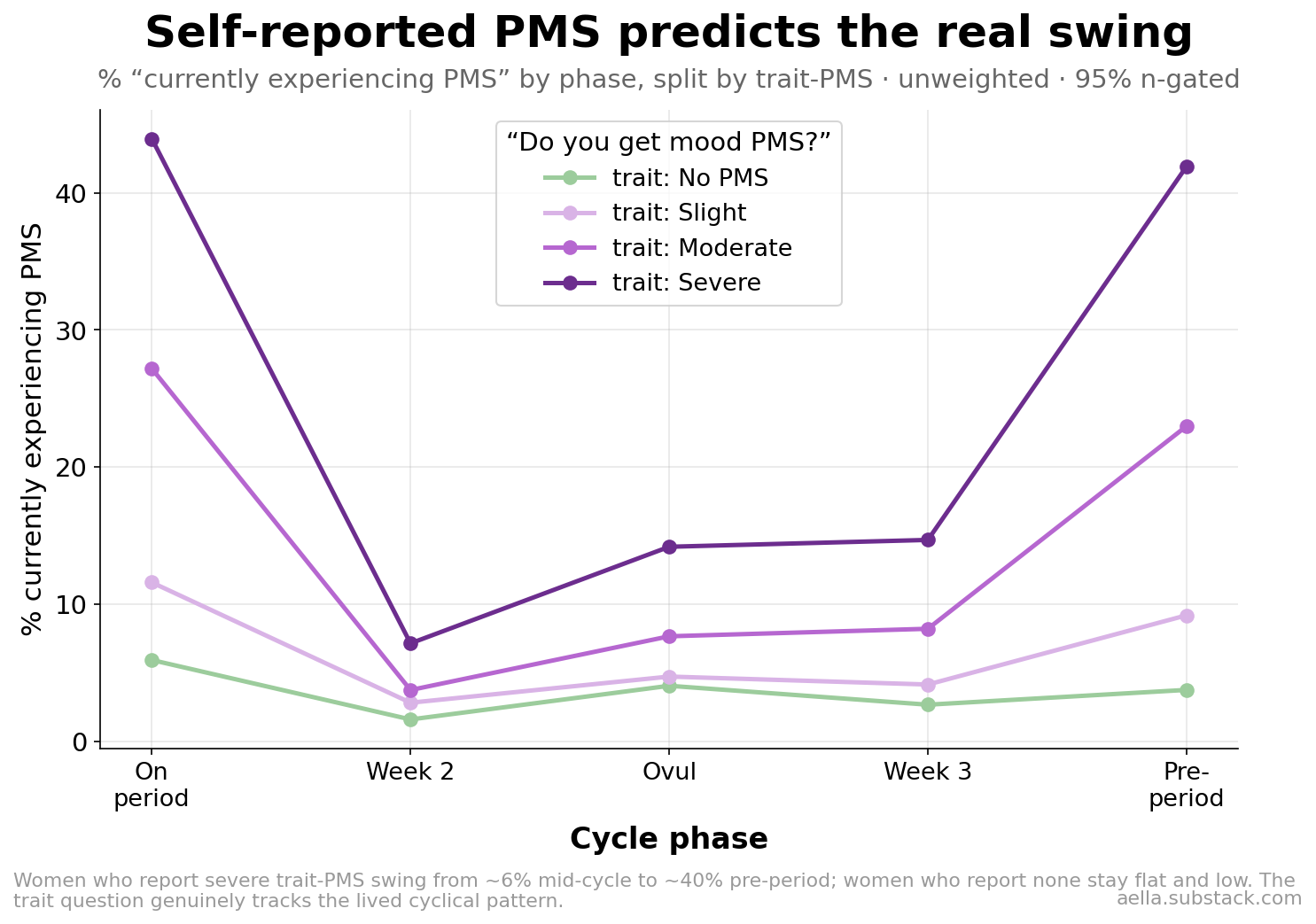
So the one-line self-report tracks the lived, within-cycle pattern. That licenses everything below — but note it's still self-report on both ends, and the cycle-phase sample is a different (smaller) subset.
03The mental-health engine
The strongest single correlate of worse PMS is mental health. Every condition we measured is associated with higher severity; the gap is largest for depression and anxiety (mean ~1.8 vs ~1.5 on the 0–3 scale).
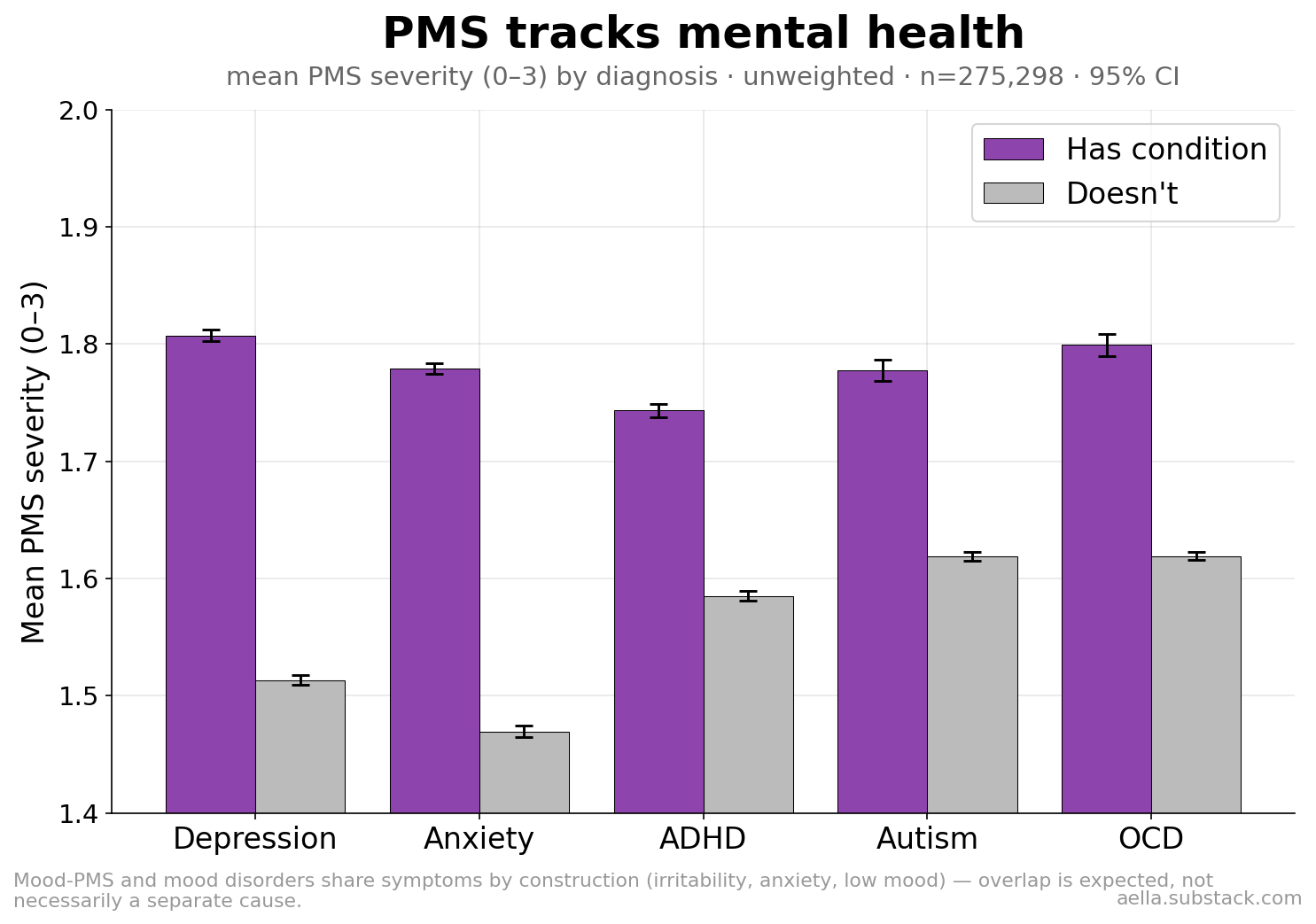
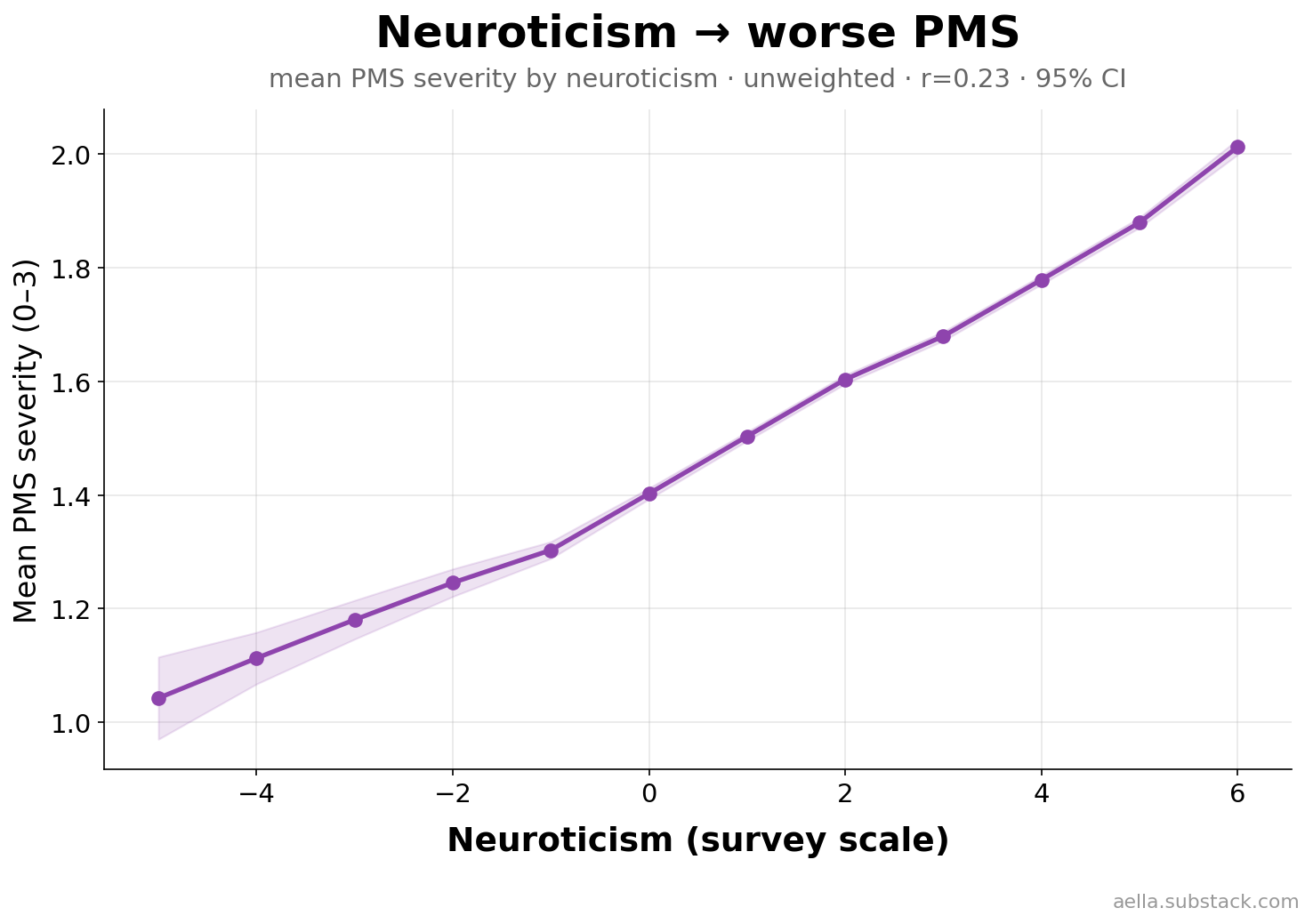
It's a smooth gradient, not a sick/well split: severity rises monotonically with neuroticism (r=0.23), the trait most about negative emotional reactivity.
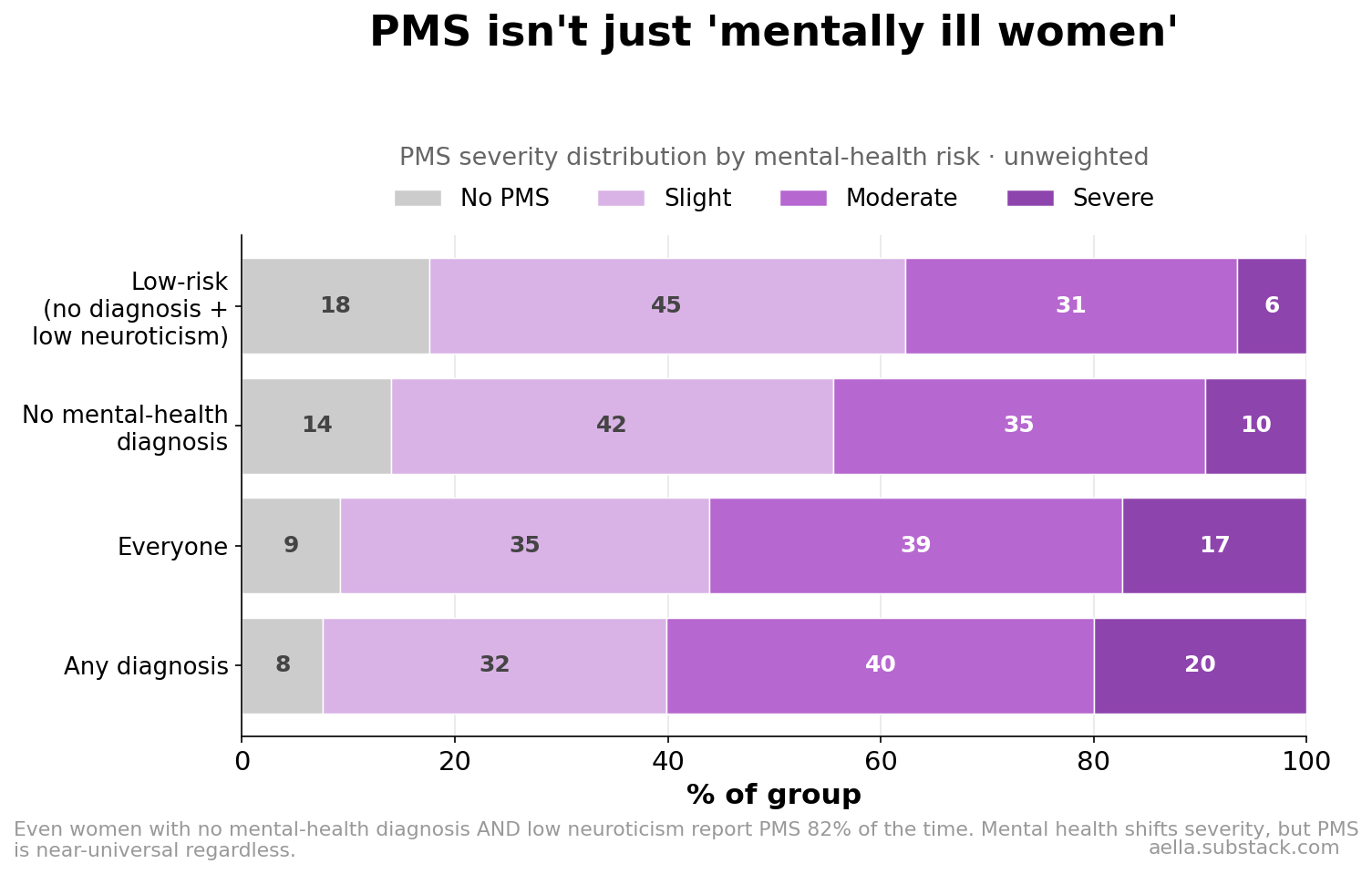
But PMS is emphatically not just "mentally ill women." Even women with no mental-health diagnosis and low neuroticism still report PMS 82% of the time. Mental health shifts the severity up — the share reporting "severe" roughly triples from the low-risk group (6%) to the diagnosed group (20%) — but the experience is near-universal regardless.
04Ethnicity — the full breakdown
A single mean per group hides the story, so here is the entire severity distribution for every ethnic group with enough data, ordered from least to most PMS.
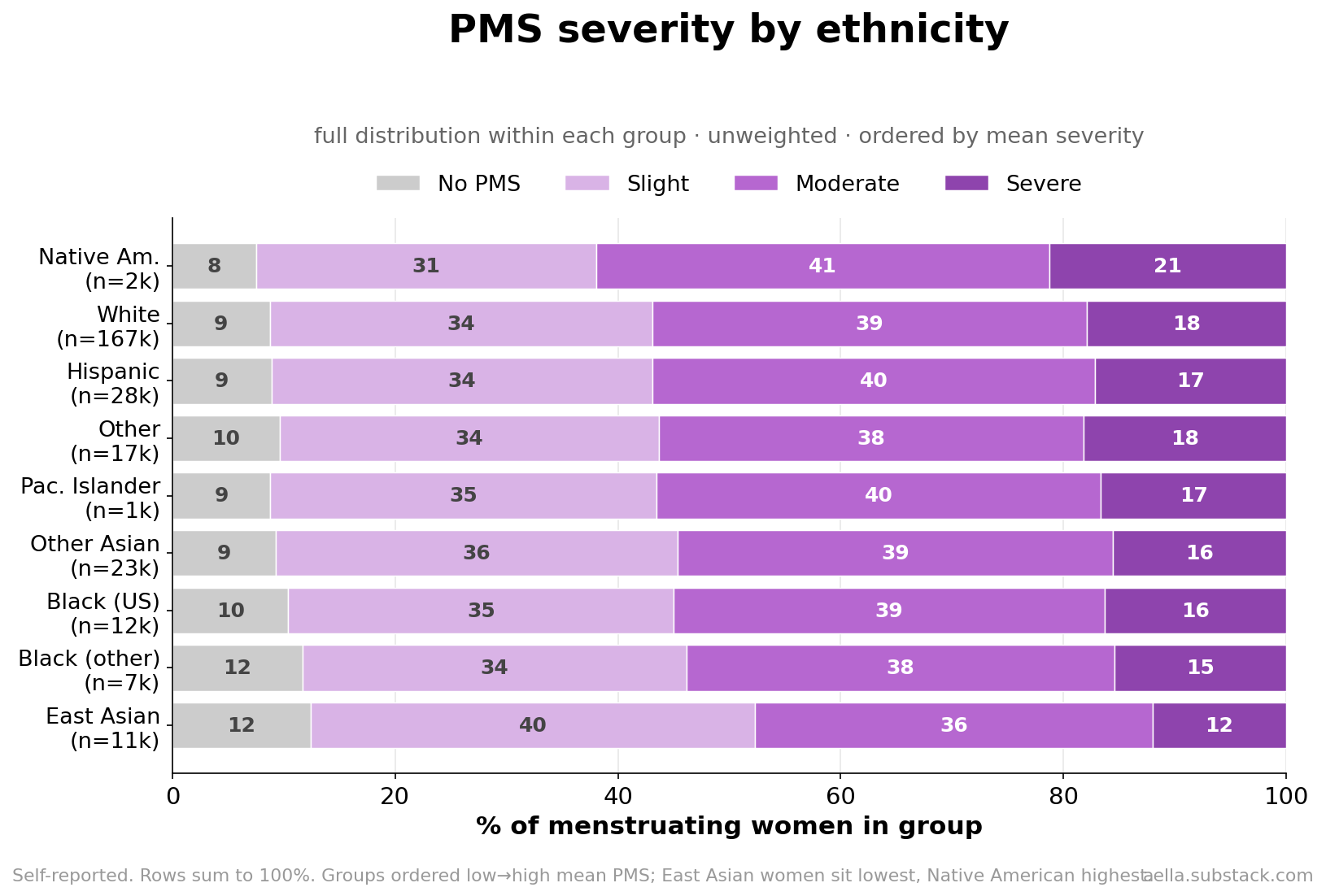
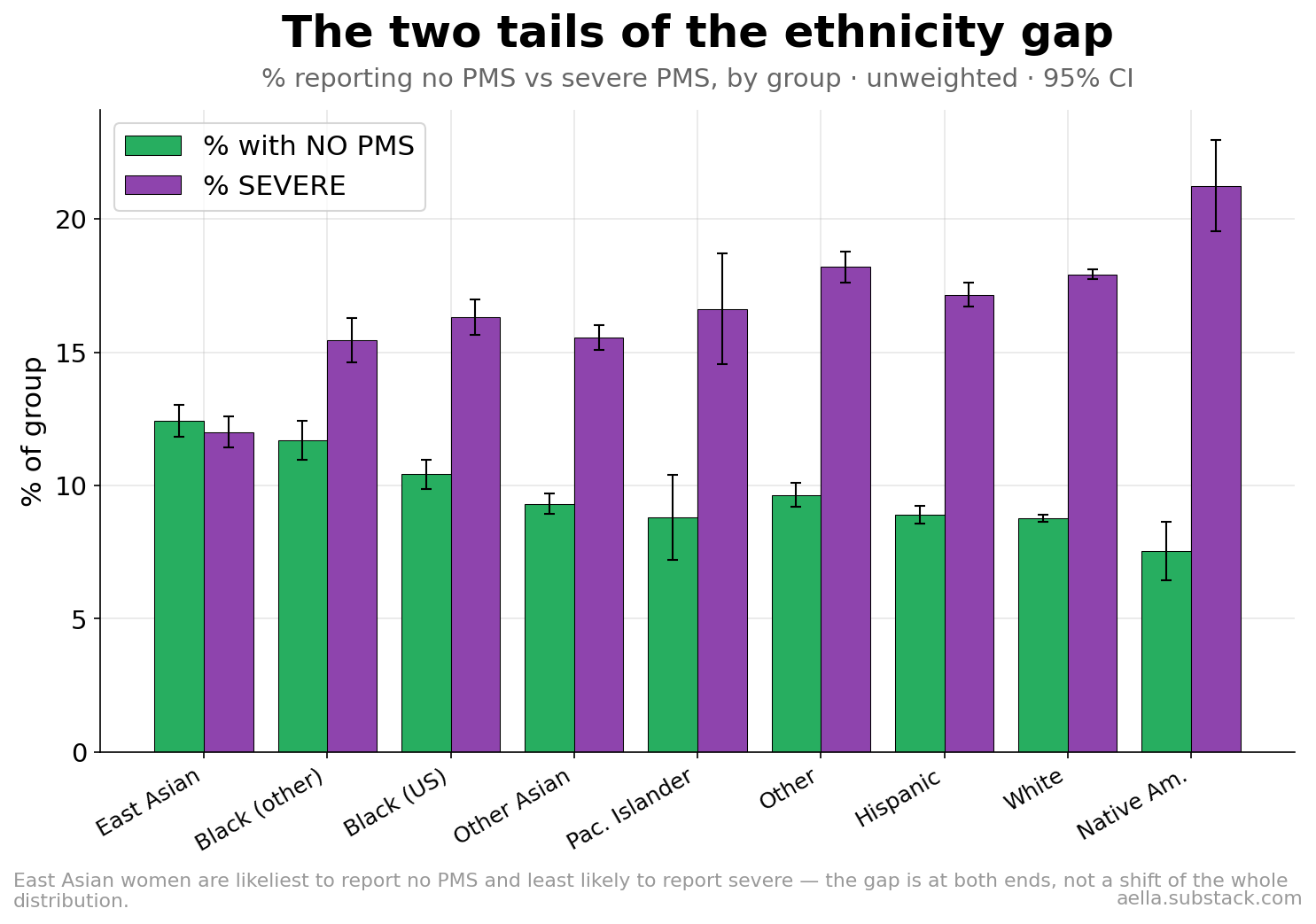
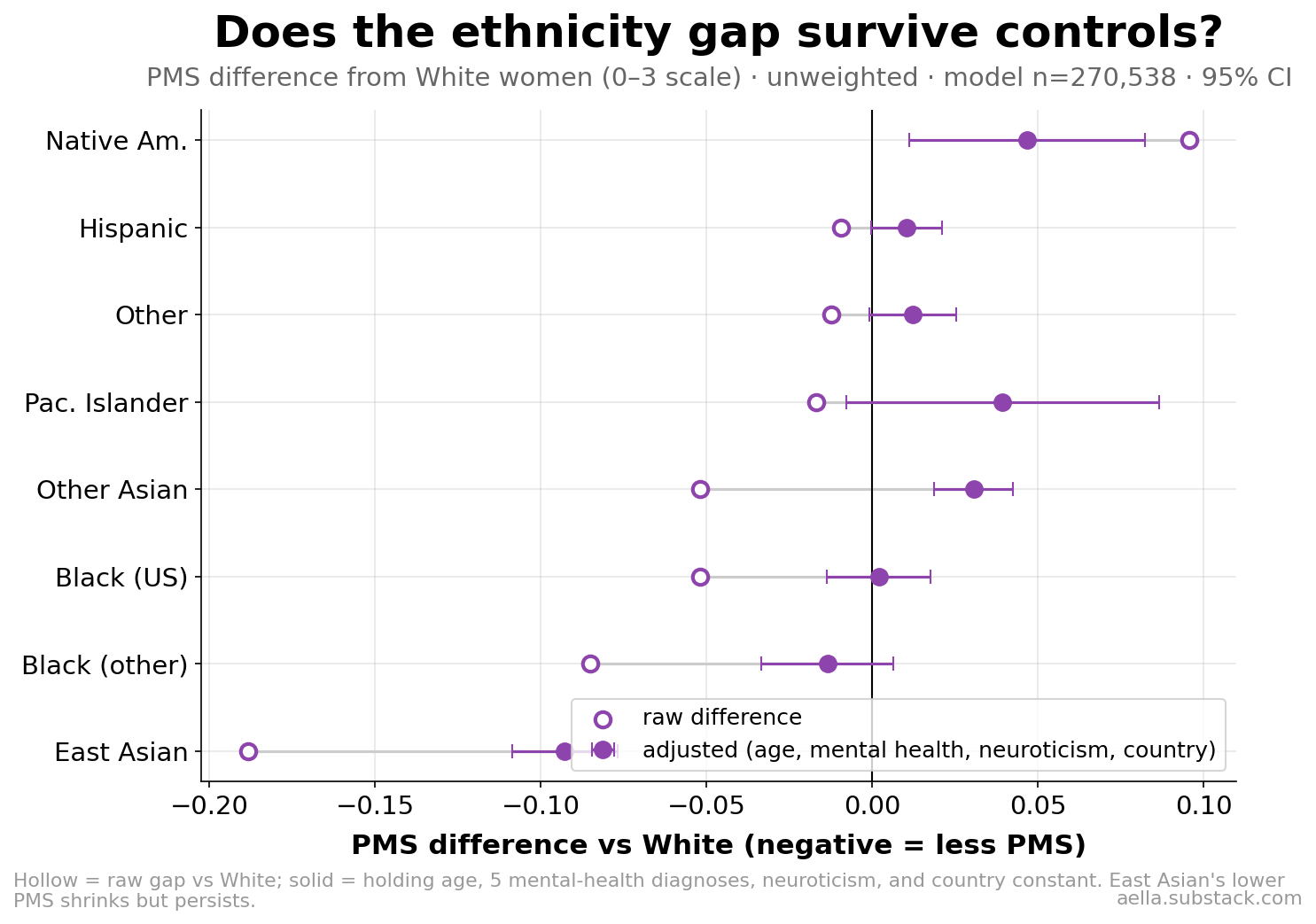
East Asian women stand out at the low end and Native American women at the high end. The East Asian difference is at both tails: they're the most likely to report no PMS (12% vs 9% for White women) and the least likely to report severe (12% vs 18%).
Is that gap just confounding — younger samples, different mental-health rates, different countries? Partly. Adjusting for age, the five mental-health diagnoses, neuroticism, and country roughly halves the East Asian gap — but it doesn't vanish.
The deeper question is whether low-reporting groups actually experience less PMS, or just describe themselves as getting it less. Here there's no regression and nothing is held constant — instead we compare two different questions the survey asks. The trait question ("do you get mood PMS?") is a one-time self-label. A separate question asks each woman whether she's experiencing PMS right now, which we line up against the cycle phase she reports being in. The reasoning: if a group genuinely has milder cycles, their in-the-moment symptoms should barely rise before their period; if they have the same monthly swing but are just less likely to call it "PMS," their right-now report should still spike pre-period like everyone else's.
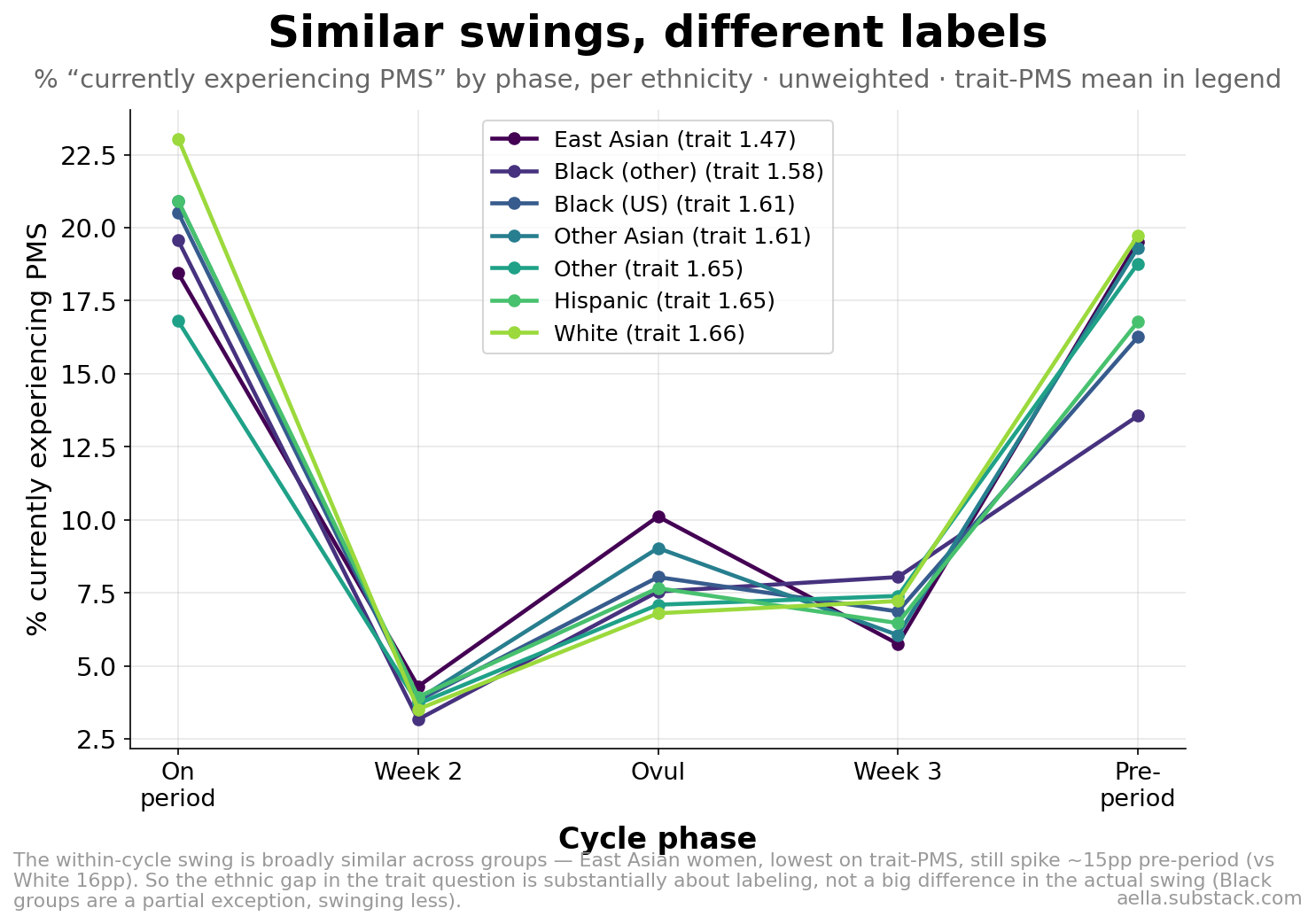
The answer: East Asian women — lowest of all on the trait question — show a near-normal pre-period spike (~15 points up from mid-cycle, vs ~16 for White women). Their lived monthly swing looks ordinary; it's the self-label that sits lower. So the ethnic gap in the trait question is substantially about labeling and threshold — how readily a group calls premenstrual mood "PMS" — not a large difference in the underlying swing. Black respondents are the exception: their current-PMS swing really is smaller (~10–12 points), so for them it looks more like a genuine difference in experience.
05Culture: religion, upbringing, country, politics
The same "real or reported" ambiguity hangs over every cultural split below — all are modest (watch the y-ranges) but consistent.
Religion
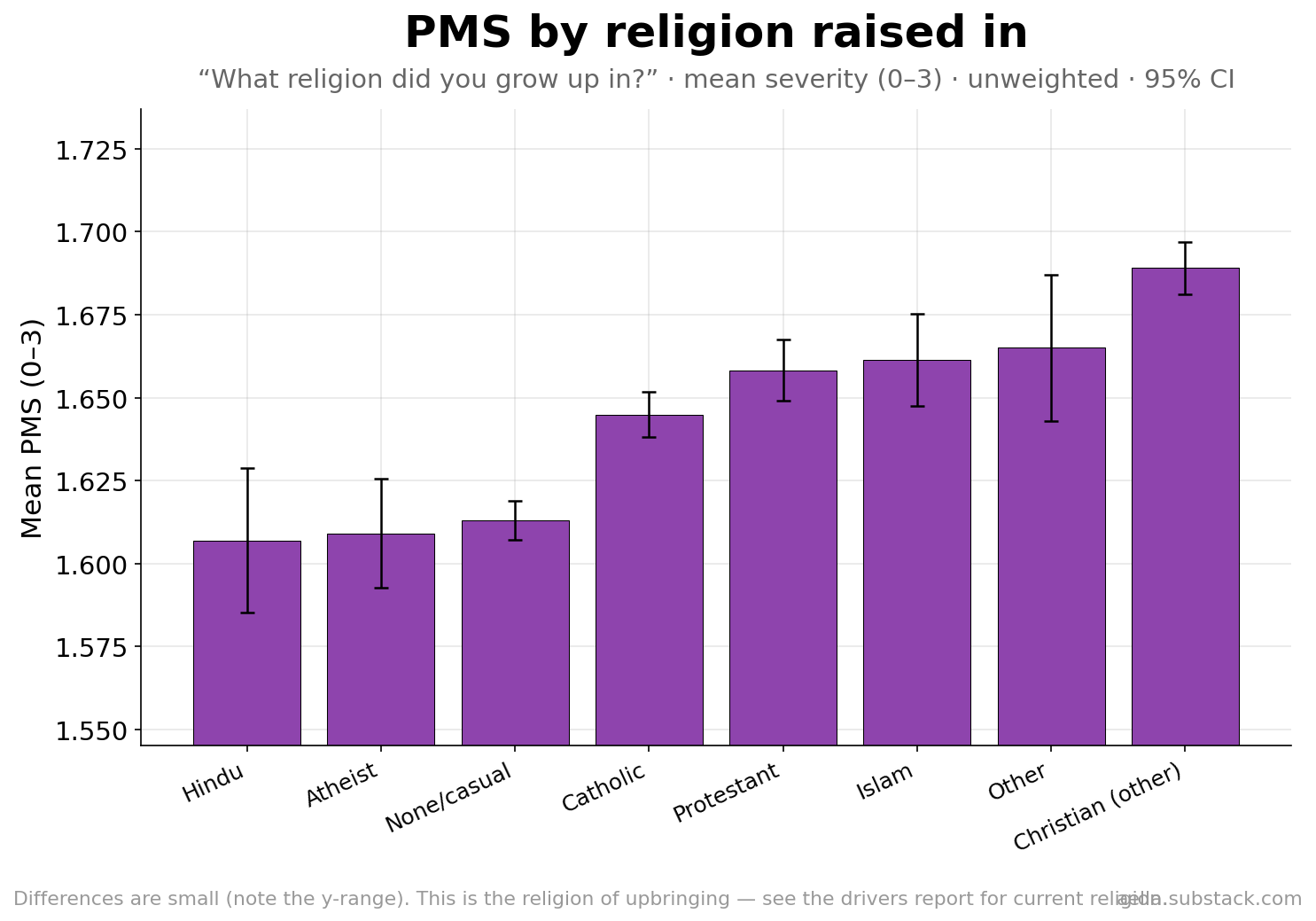
By the religion a woman grew up in ("What religion did you grow up in?"), differences are small: those raised non-religious, atheist, or Hindu report slightly less; raised "other Christian," Muslim, or "other" slightly more. For the deeper question — religion vs class vs temperament, type-of-religion at equal religiosity, and apostasy — see the companion PMS drivers report.
Upbringing & religiosity
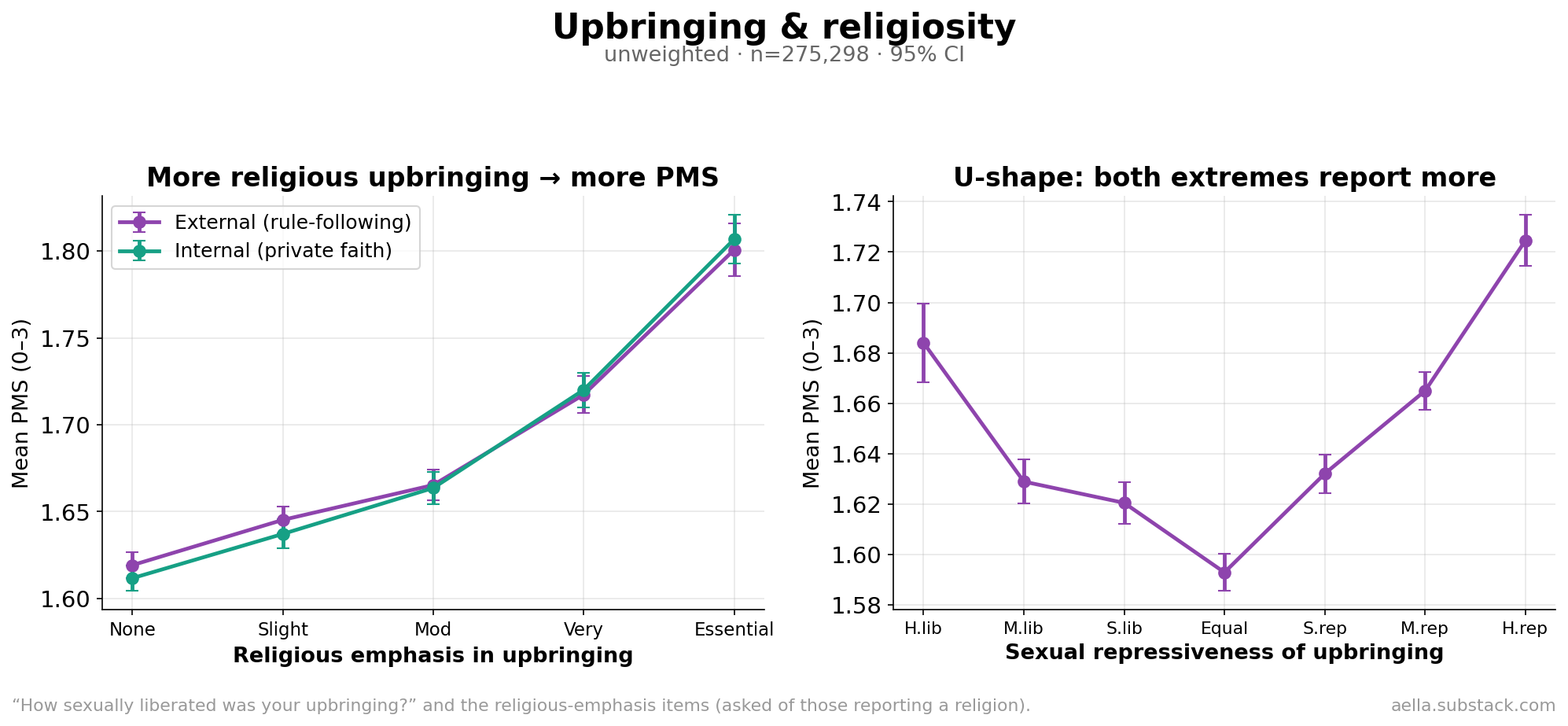
Two clean patterns. The more religious the upbringing, the more PMS — a monotonic climb from 1.62 (no religious emphasis) to 1.80 (religion "absolutely essential"), and internal vs external religiosity track each other almost exactly. And the sexual repressiveness of upbringing is U-shaped: women raised in the most repressed and the most liberated environments report more PMS than the balanced middle.
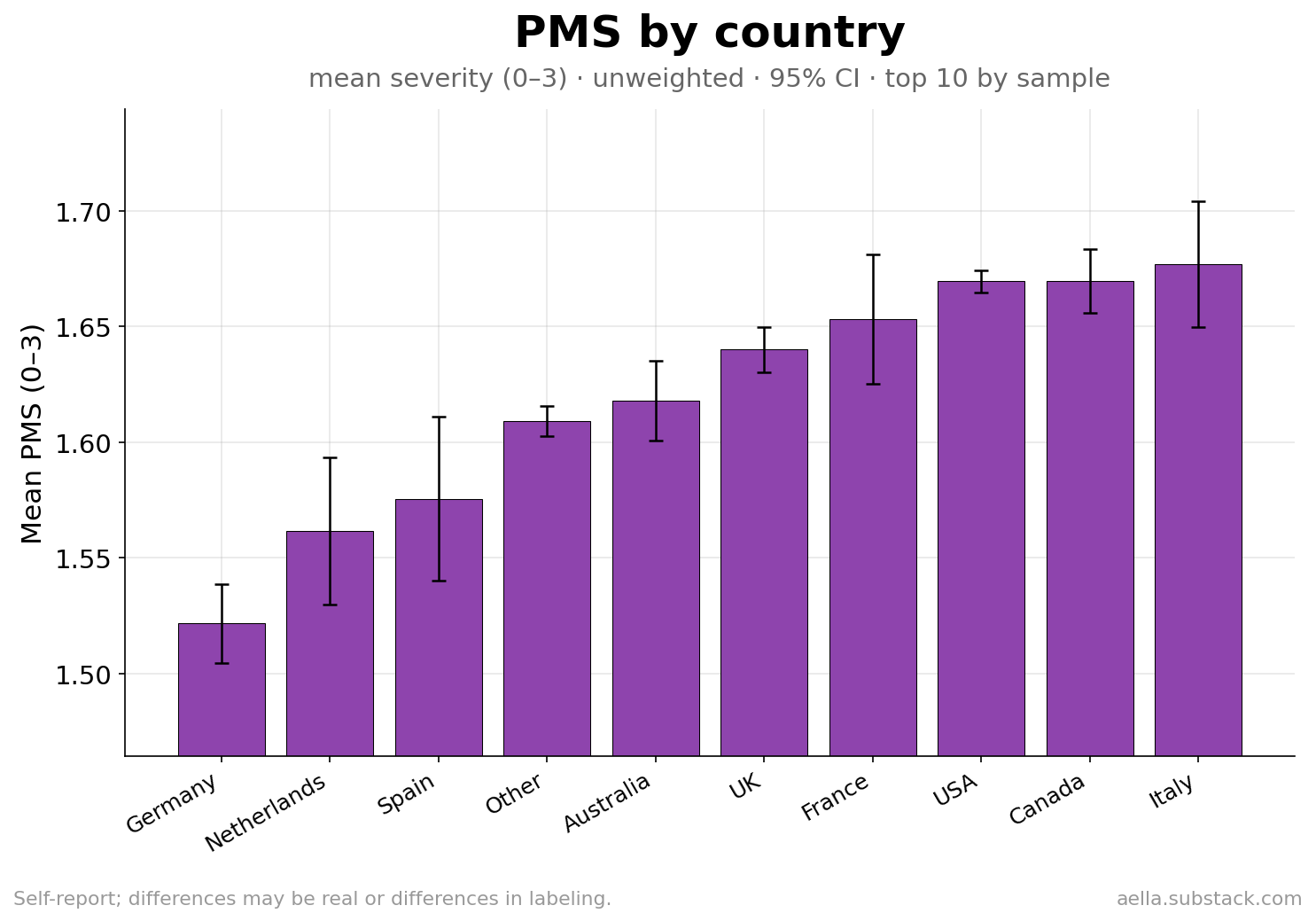
Country
Among the ten largest country samples, Germany, the Netherlands, and Spain report the least PMS; the US, Canada, and Italy the most — echoing the ethnicity pattern and again plausibly a mix of real difference and reporting culture.
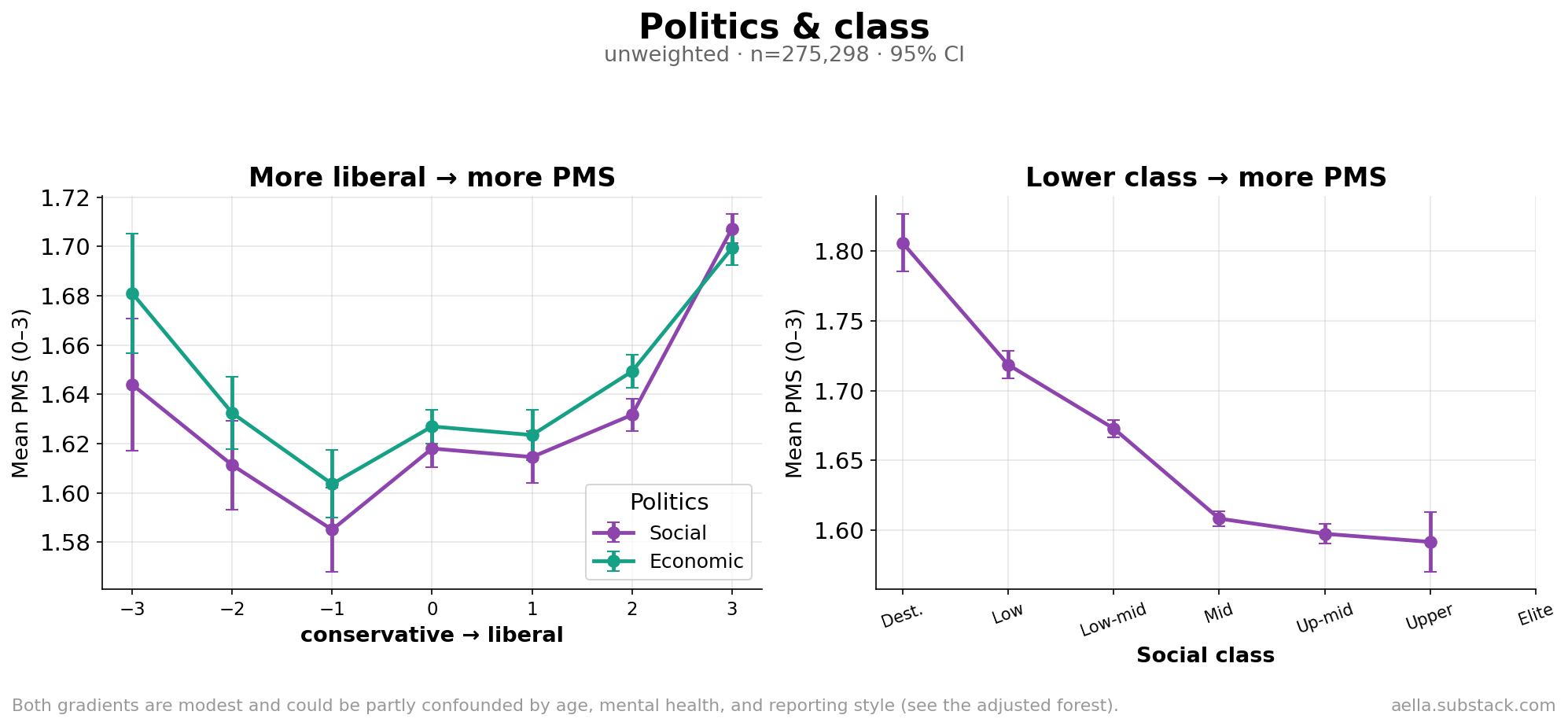
Politics & class
More socially and economically liberal women report more PMS (with the very-liberal end highest), and lower social class tracks more PMS. Both are modest and, as the next section shows, mostly explained by other factors.
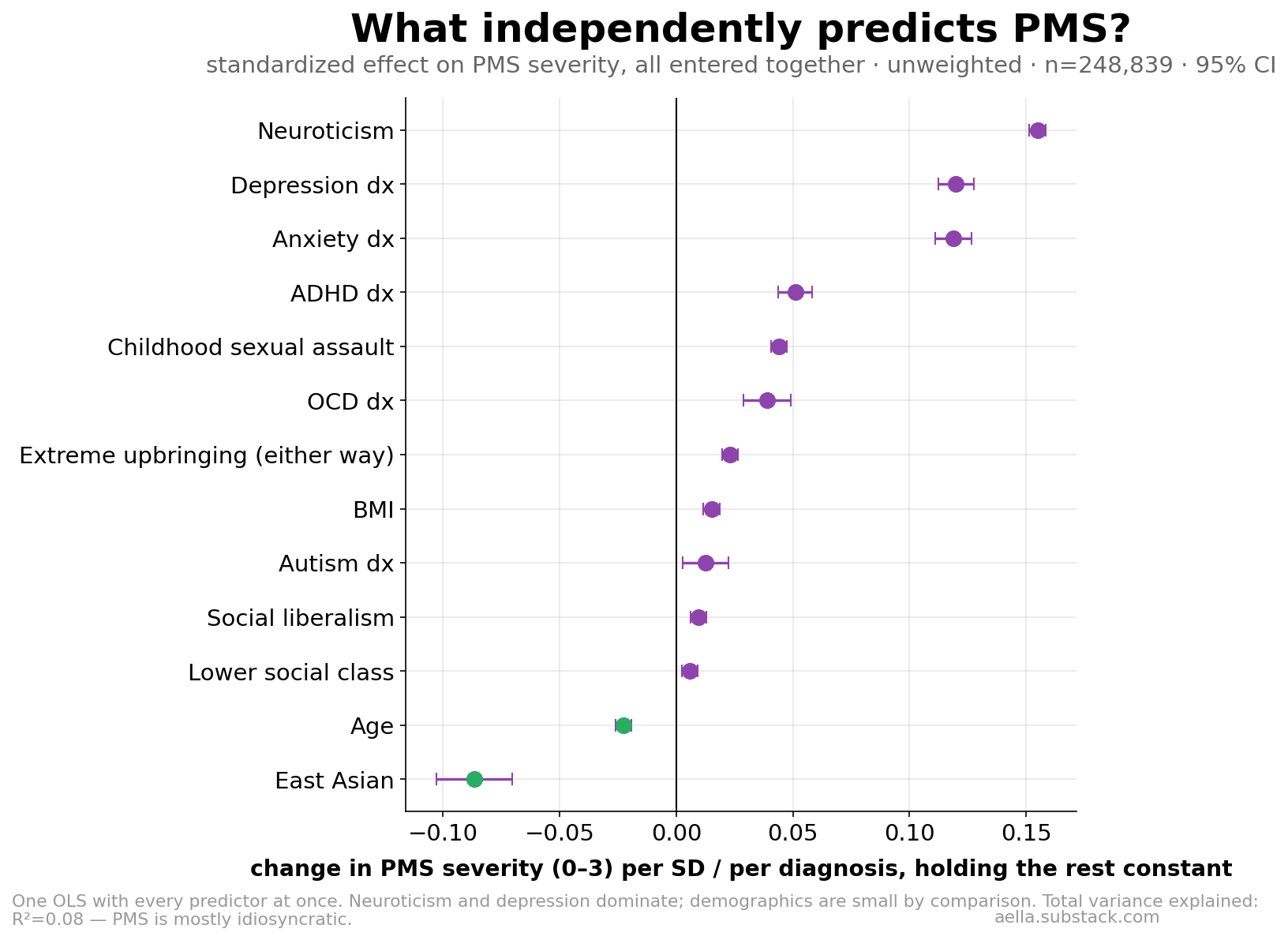
06What actually predicts PMS, all at once
Throwing every predictor into one model — to see which matter holding the rest constant — settles the hierarchy. Neuroticism and depression dominate; anxiety, ADHD, childhood sexual assault, and OCD follow; and the demographic effects (extreme upbringing, liberal politics, class, BMI) are small once mental health is accounted for. The biggest demographic coefficient is East Asian ethnicity (protective).
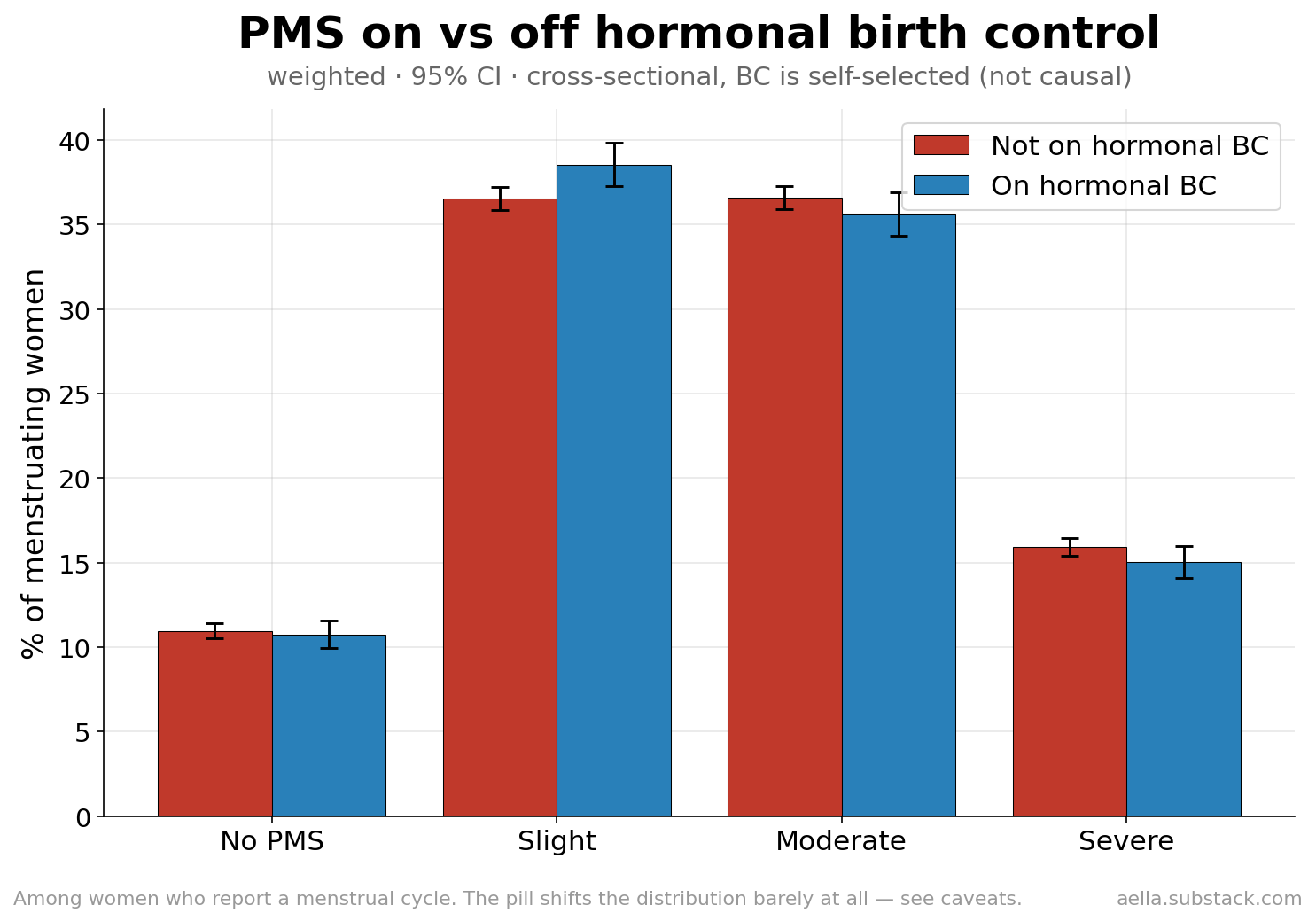
07Does the pill help? (Barely, here)
A common belief is that hormonal birth control smooths out PMS. In this cross-section it essentially doesn't: women on hormonal BC report almost the same severity distribution as women not on it (15.0% vs 16.0% severe).
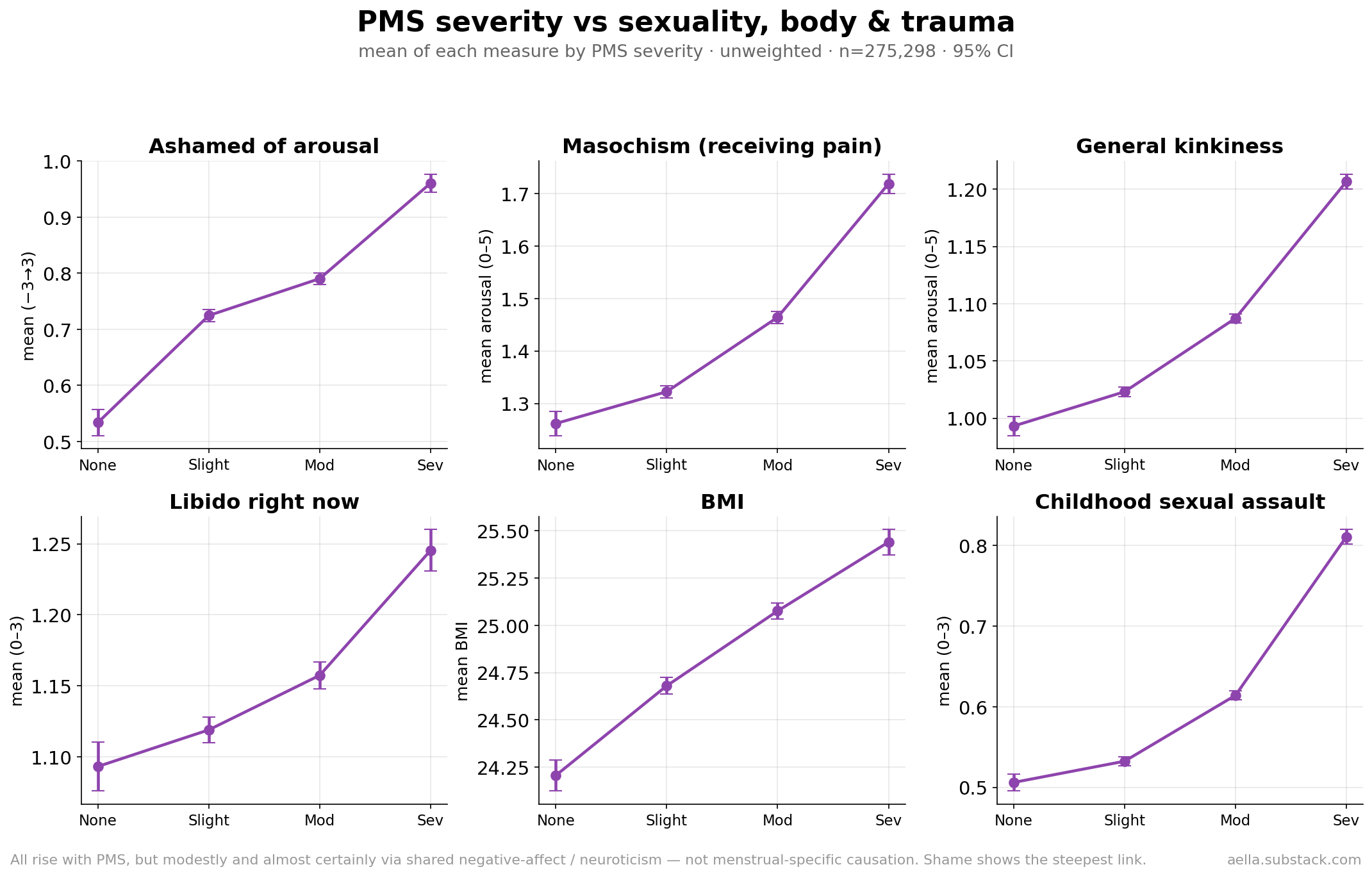
08PMS, sexuality & body
Because this is a kink survey, we can connect PMS to sexuality. Everything rises gently with PMS severity — women with worse PMS are more ashamed of their arousal (the steepest link), somewhat more into masochism and kink generally, slightly hornier in the moment, a bit higher in BMI, and report more childhood sexual assault.
09Methodology & limitations
Source & measures
Aella's Big Kink Survey (GuidedTrack), menstrual block added Nov 2024, n=1,071,355 total. The trait PMS item — "Do you get mood-based PMS symptoms during your menstrual cycle? (e.g., irritability, anxiety, depression)" — is coded No=0 / slight=1 / moderate=2 / severe=3; "I don't menstruate / I don't know" is excluded, not coded 0. The validation in §2 uses two further items: "Are you currently experiencing PMS symptoms?" and "Where are you currently at in your menstrual cycle?" Analysis is restricted to natal-sex-Female respondents (incl. nonbinary AFAB) not flagged as pregnant.
Base rates use population raking weights (sex/age 14–33/cis-trans/politics/BMI/ethnicity; eff. n≈54k). All breakdowns and models use the full unweighted sample (n=275,298 with a PMS answer; model n=248,839 after dropping missing covariates) — precision over representativeness, per the chaosfactor convention. The adjusted forest is one OLS on standardized predictors; the ethnicity-adjusted chart controls age, five MH diagnoses, neuroticism, and country. Bars/bands are 95% CIs.
Limitations
- Mood symptoms only — no physical-symptom measure, so total PMS burden is undercounted.
- Self-report & symptom overlap — the mental-health correlation is partly built into how both are measured. §2 shows the trait item is nonetheless valid against the cycle pattern.
- Reporting vs experience — the ethnicity and country differences are partly about labeling, as §4 argues; this survey can't fully separate the two.
- Not representative — the sample is self-selected and skews young, online, and Western (the survey spread virally, well beyond Aella's own following); weighting fixes demographics, not selection. The pill analysis is cross-sectional and self-selected, not a treatment effect.
- Cross-sectional throughout — no woman is followed across her own cycle; phase comparisons are between different women.
Analysis pipeline: pandas + numpy; scripts and full tables available on request.